

Much has been made of the Swedish approach to the COVID-19 pandemic, unique among European nations for implementing relatively few restrictions. While other countries closed everything down and wore masks when returning to public spaces, Swedes were eating out and getting mask-less haircuts (although in groups less than 50 and avoiding their grandparents.) The ‘COVID is a conspiracy folks’ love to cite Sweden as an example of sane policy, while most of the public health folks I know were sad that one of their favourite examples of a successful social welfare state could be so careless. In all likelihood, it will be another year before we have all the information needed to understand which approach was best, and why.
In Sweden the policy has been set by scientists and not by politicians. Anders Tegnell, head epidemiologist at the Swedish Public Health Agency, has been the face and voice of the Swedish Policy, and from the beginning has prioritized the long-term sustainability of pandemic response, considering citizens’ capacity for altrusim/compliance, the sustainability of requests, and the ripple effects of shutdown measures on social determinants of health driven by the economy.

Although high schools and post-secondary switched to online in March, Sweden never shut down elementary schools. The childcare benefits of schooling young kids was seen as an essential pre-requisite for their parents to work productively; I’m betting we will find that this policy reduced a lot of the gender imbalances in work productivity/performance that is seen in academia, for example.
In the Autumn, high schools and post-secondary came back online. While my prof colleagues elsewhere were preparing zoom lectures, Swedish Universities collectively took a decision to come back to campus – inclusive of frosh parties(!) At KTH, there were some space constraints to bring all students back and into bigger classrooms to allow for distancing between them. So, it was decided that first year classes would have priority for on-campus learning. Fourth year students would have next priority so that they can finish up, and students in the middle were determined to know enough about the system that they’d be fine with a mostly online experience. I teach only graduate courses, and have a mix. All my teaching is ‘room+zoom’, with an in-person component and and some students dialing in on web conference, either because they don’t feel well, or they are in a high-risk group. This means I head into campus 1-2 days per week, and things are pretty quiet when I get there since most folks (students and faculty) are opting to do most of their work from home.
This week I gave a lecture on how COVID-19 can (or has) influenced workplace design, in some cases requiring installation of barriers or changing the organization of work. Most of my examples came form from North America, partly because of my attention to that area, spending the first part of the pandemic there, my media diet, and also… many of the examples I gave have not ben implemented here, or not the the same degree.
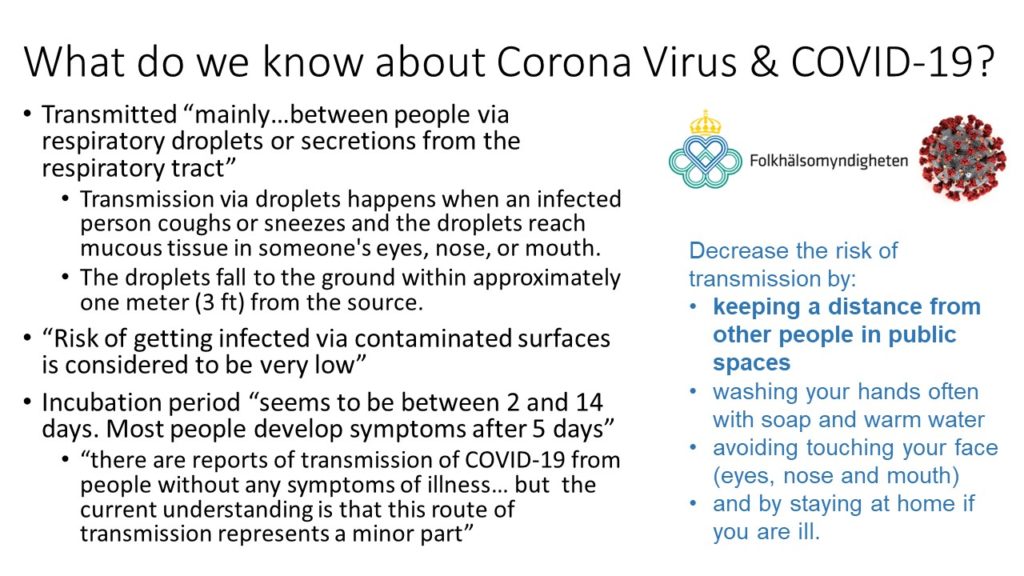
One of the slides presented is above, and it shows excerpts of the information given on the Swedish Public Health Agency website. Many researchers and academics will call for ‘evidence-based practice’ in any situation; in cases where the evidence is incomplete or inconclusive, decisions should be made on the best available evidence. In unknown areas, some will default to the precautionary principle and seek to avoid risk even before (or if) there is definitive proof that something is hazardous. Many of the EU (and Swedish) approaches to environmental and occupational chemical exposures are precautionary… so it is a surprise that Sweden is not promoting all available risk reduction strategies.
This brings us to masks. In Canada masks have been recommended for some time, and there have been North American attempts to promote the use of masks by describing, like the video below, more clearly how and why they help. They are very low cost, and using the weak evidence of ecological studies, countries that have implemented them widely have better control of the virus. I’m not about to wade into the conspiracy minefield of angry anti-mask folks (apparently wearing a mask is ‘slavery’ but wearing your tinfoil hat is A-OK).
In usually precautionary Sweden, mask use is super infrequent. As my supervisor puts it “you really only see them on foreigners on the subway”. (Side note: IT ME.) This is one part of the Swedish policy that does not make sense to me; the infection control advice seems to be stuck back in March. As seen in the presentation slide, there is acknowledgement that contacting surfaces is not a common route of transmission, but 2 of the 4 infection control directives are related to this route: wash your hands and don’t touch your face. There is acknowledgement that infection can be spread by asymptomatic people (WHO is pretty clear that you can spread before you have symptoms, or if you have some symptoms but don’t feel sick) …so the directive to ‘stay at home when you feel ill’ doesn’t seem like enough.
The main argument against masks here seems to be: if we tell people to wear masks, they will stop taking all other precautions. Welp, as Frosh Week indoor karaoke parties demonstrate, folks are not all that diligent about the ‘other precautions’. Lots of folks are avoiding transit and avoiding peak times, but I have been on a few standing-room only cars where 10cm between folks is impossible, let alone 2m. While I’m not an expert in the social psychology of Swedes, I disagree that seeing a crowd of masked people will induce crowding and risk taking. If anything, masks are a continual reminder that things are not ok, or normal. From my own personal experience of wearing one on transit and the grocery store, people do not rush towards me feeling all safe due to my cotton germ-strainer. On the contrary, when I walk onto a subway car wearing a mask, people back the fuck up. For folks who are not crushed by social censure (it also me!), this is actually a bonus way to have some extra space. Once in a while I see another mask person, and a few times have had a wink or smile or nod recognizing a fellow germ-wrangler.
This is already a super long post (perhaps because I’ve put off finishing it!), but I’d like to also add a comment based on an article by Indi Samarajiva that has really stuck with me (thanks to lovely USask colleague Erin for the recommendation!) Many of the international comparisons of pandemic response in English media have focused on the UK, US, Sweden, New Zealand…. all countries with mostly white people. Its interesting to notice that some strong suppression of the virus has been in Asia, and some countries in Africa and the Caribbean are doing an amazing job… even more so when considering their public health budgets and overall GDPs are much lower than some of the nations they are outperforming (cough cough USA). I am really grateful to Indi and everyone interpreting the pandemic with a race, or gender, or class lens.